When Every Agency Says “No Authority,” America Has a Public-Health Blind Spot
Patient voices, diagnostic access, environmental illness, and the homeland-security cost of ignoring families in collapse—Guest Opinion by Billie Glazier
Guest Opinion by Billie Glazier
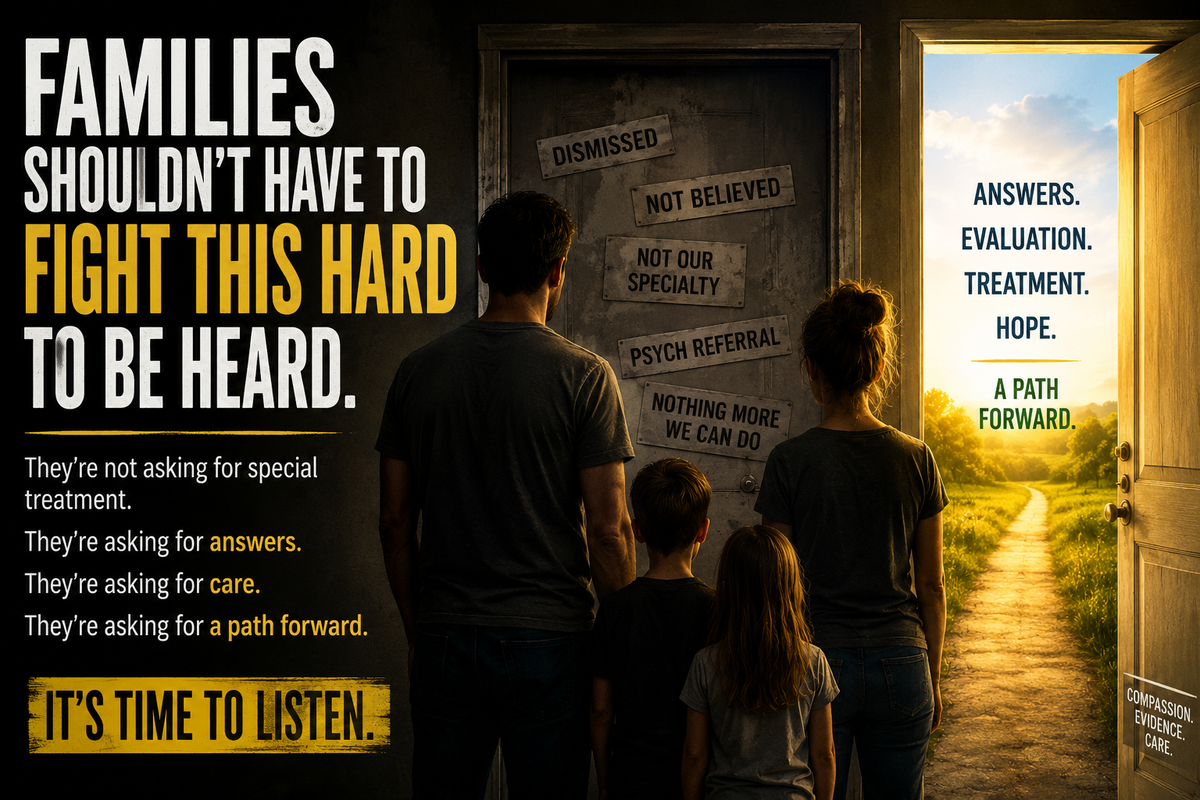
There is a category of American families that America’s healthcare and public-health systems do not know how to hear.
They are families dealing with suspected parasitic disease, mold-related illness, fungal infection, environmental contamination, and complex infectious symptoms that do not fit neatly into a ten-minute appointment or a standard lab panel. Many are not asking for a predetermined diagnosis. They are asking for the most basic things a functioning health system should provide: a serious evaluation, appropriate testing, competent review of evidence, and a clear pathway to care.
Instead, too many are dismissed, redirected, labeled, and abandoned.
Across affected communities, families describe the same pattern. They ask for parasite testing and are refused. They request infectious-disease evaluation and cannot find a referral pathway. They submit photographs, videos, specimens, timelines, and environmental histories, only to be told that the material will not be reviewed. When medication is offered, families often report narrow, short-term prescriptions that do not address species identification, source control, co-infections, environmental exposure, or family-wide risk.
Then the families deteriorate. Jobs disappear. Homes are lost. Children are pulled out of normal life. Parents become investigators because the institutions funded to investigate have closed the door.
The usual explanation is that these patients are anxious, delusional, noncompliant, or confused. Mental-health care has its place. But psychiatric labeling must never become a shortcut around infectious-disease evaluation, environmental review, or diagnostic humility. When a patient reports parasites, mold, fungal disease, or contamination, the first institutional response should not be stigma. It should be evidence review.
The “No Authority” Problem
When affected families reach beyond the clinic, they encounter the same institutional dead end. Health departments say they have no authority. Federal agencies say they have no authority. Environmental offices say they have no authority. Elected officials refer families back to the same medical system the families are reporting as inaccessible or abusive.
A system that cannot receive a warning cannot respond to a threat.
When an agency lacks authority, it should identify who has it. When a public-health report falls outside one office’s jurisdiction, it should be transferred to the correct office. When citizens report possible biological, fungal, parasitic, or environmental threats affecting homes, animals, children, farms, vehicles, and communities, the answer cannot be a dead-end phone call.
This is not only a healthcare issue. It is a surveillance issue. It is a preparedness issue. It is a homeland-security issue.
Affected families are now doing the pattern recognition that institutions should have done. They are collaborating across states, comparing medical records, documenting repeated refusals, identifying patterns of medical gaslighting and abandonment, and asking why the country has no visible intake channel for parasitic, fungal, mold-related, or environmental biological threats that do not respect property lines.
In my own advocacy, my tally across affected networks identified more than two million families that cannot find help, and that number is expanding daily. These are not merely individuals. They are families: parents, children, spouses, grandparents, caregivers, workers, students, and entire households watching their families implode.
Even more disturbing: despite searching affected communities, we have not found one clear example of a family receiving comprehensive, integrated, accountable care for the full pattern they are reporting. If that care exists, public officials should want to identify it, replicate it, and scale it. If it does not exist, they should want to know why. But so far not a single leader we have approached as asked a single question or intervened meaningfully.
This Article Only Scratches the Surface
This article discusses only the surface of a deeper structural problem.
The reports we have repeatedly submitted to institutional gatekeepers do more than describe suffering. They expose existing dots and the deadly connections that bridge them: inaccessible diagnostics, agency dead ends, public-health undercounting, fragmented authority, conflicted policy formation, misaligned appropriations, and families deteriorating while the institutions funded to protect them disclaim responsibility.
One dossier submitted for Congressional review, The People’s Dossier, Part I, presents a structured analysis comparing parasitic disease burden with national healthcare spending among peer high-income nations.
Using Institute for Health Metrics and Evaluation 2023 age-standardized DALY data and World Bank 2022 health-expenditure data, that dossier reports a positive association within a seven-country OECD high- income comparison group between per-capita healthcare spending and parasitic disease burden. The United States sits as a high-spending outlier with unresolved burden that is not proportionate to its level of tax-dollar investment. The more we fund the issue, the bigger it expands, and the more it grows, the larger the allocations—while reporting pathways are shut down and there exists no tangible benefits.
This regression analysis raises a direct appropriations question: whether escalating disease burden is being converted into institutional funding without proportional improvement in detection, treatment, surveillance, or public protection.
That is the public-health version of a money machine that sacrifices American lives and our children’s futures for industry profits.
The bigger the unresolved problem becomes, the more funding the system can request. The more funding the system receives, the larger and more entrenched the system becomes. But if that funding does not reach diagnostic pathways, parasitology expertise, fungal evaluation, environmental review, citizen-reporting channels, or rescue for families already in collapse, then the public is not funding solutions. It is funding the appearance of response while the burden grows.
Congress should ask a blunt question: are CDC, HHS, CMS, and related public-health programs using taxpayer dollars to reduce disease burden, or are they merely documenting, managing, and expanding around it?
Compared with peer nations with similar income per person, the United States is sitting high on a hill of spending and disease. In a functioning system, more funding should buy earlier detection, stronger laboratory capacity, better specialist access, more accurate surveillance, and lower preventable burden. For affected families, the lived experience is the opposite: more bureaucracy, more referrals into nowhere, more records used against them, and fewer meaningful pathways to answers.

MAHA Is Moving the Conversation, But Patients Must Be in the Room
The Make America Healthy Again effort is making progress, and this article should not be read as an attack on that project. MAHA has moved national attention toward root causes, chronic disease, food quality, environmental exposure, medication overuse, transparency, and conflicts of interest. Those issues matter.
But one factor healthcare reform repeatedly omits is the patients’ voices.
That omission is not minor. It is the structural flaw that allows reform to be designed around patients without being informed by patients. It allows institutions to discuss chronic disease, environmental exposure, overmedicalization, public trust, and regulatory capture while excluding the families living inside the consequences.
When medical policy leans primarily on the medical industry during formation, government is handing the pen to the very people with the highest and most complex conflicts of interest. Industry input may be necessary. It cannot be the only input. It cannot be the controlling input. And it cannot be treated as neutral when the same system being consulted is the system patients are reporting as harmful, dismissive, financially conflicted, and procedurally inaccessible.
That mentality is why affected people and parents of ill children are no longer apologizing for our tone while trying to save our babies.
We are not asking for politeness to be confused with credibility. We are asking for facts, testing, review, independent expertise, and accountability. Parents watching children deteriorate should not have to soften every sentence to make institutional gatekeepers comfortable. The urgency is not the problem. The suffering is the problem. The abandonment is the problem. The missing pathway is the problem.
Patients are not anecdotes. Parents are not noise. Families are not public-relations problems. They are evidence of the systemic failures that the system has been trained to ignore.
The Political Failure Is the Absence of Basic Questions
We have reached out to public officials, including Alabama Attorney General Steve Marshall, Representative Robert Aderholt, Representative Barry Moore, Senator Katie Britt, and Governor Kay Ivey. The most troubling part has not been only the absence of help. It has been the absence of basic questions.
When families say children are deteriorating, when they offer documentation, images, specimens, timelines, and patterns, public servants should ask questions. They should want to know who has jurisdiction. They should want to know whether agencies are tracking similar reports. They should want to know whether Alabama families, and families across the country, are falling through a structural gap.
Silence is not neutrality when lives are at stake.
This is not a partisan issue. Parasites do not care how someone votes. Mold does not respect party affiliation.
Fungal threats do not stop at county borders. Environmental contamination does not pause while agencies debate jurisdiction. Disease burden falls on conservative families, liberal families, rural families, urban families, veterans, children, and people who have never asked anything from government except a fair chance to survive.
The Homeland-Security Blind Spot
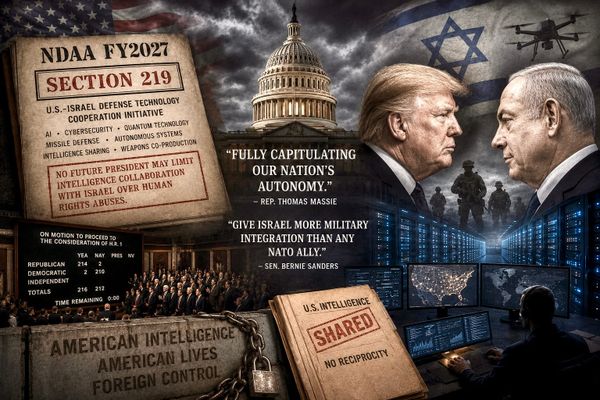
The United States already understands that biological materials and environmental pathogens can raise national-security concerns. In 2025, federal prosecutors in Michigan charged two Chinese nationals in connection with the alleged smuggling of Fusarium graminearum, a crop-damaging fungus described by the Justice Department as a dangerous biological pathogen and potential agroterrorism concern. Later, one researcher pleaded guilty to smuggling a biological pathogen and lying to FBI agents.
This point should be handled carefully. It is not an argument against foreign scientists. It is not an argument for panic, prejudice, or speculation. Reporting also noted disputes over the practical risk and did not establish malicious intent by every person involved. The lesson is narrower and more important: federal authorities already treat unauthorized biological materials as a security issue when they appear at the border or in a lab.
Why, then, are American families unable to find a clear pathway when they report possible biological, fungal, parasitic, mold-related, or environmental threats in their homes, farms, bodies, and communities?
The answer cannot be that no one has authority.
A country cannot defend against threats it refuses to see. Homeland security does not begin after a crisis is confirmed. It begins with intake, evidence preservation, pattern recognition, testing, escalation, and accountability. If the public has no functional channel to report credible biological or environmental warnings, then the country’s early-warning radar is essentially shut down.
That vulnerability can be exploited by time, nature, negligence, conflict of interest, or adversaries. The source matters. But detection comes first. Without a public health radar, our homeland security is a gapping vulnerability in the face of bioweaponry.
The Demands Are Direct
Affected families are not asking for sympathy. We are demanding action.
First, we demand rescue of the suffering families. That means immediate access to qualified diagnostic evaluation, appropriate parasitic and fungal review where indicated, environmental-health assessment, specimen intake, safe documentation channels, and emergency stabilization for families whose homes, bodies, animals, and children may be affected by unresolved biological or environmental threats.
Second, we demand restitutionary funding for families who have lost jobs, homes, income, education, safety, and stability because medical abandonment and agency failures left them untreated, unprotected, and financially destroyed. These are not ordinary private hardships. They are the foreseeable costs of a system that refused to evaluate evidence and then left families to absorb the consequences alone.
Third, we demand Homeland Security meetings to close the obvious vulnerabilities created by these failures.
If families cannot report suspected parasitic, fungal, mold-related, environmental, or biological threats through any clear public channel, then America’s early-warning system is broken. Homeland security leaders should meet directly with affected families, independent experts, ethical clinicians, environmental specialists, and public-health officials to identify and close those gaps.
Fourth, we demand accountability with criminal consequences where the evidence supports it. That includes providers, administrators, institutional actors, and outside pressures that knowingly falsify records, obstruct care, retaliate against patients, suppress evidence, coerce silence, or contribute to preventable deterioration through conduct that meets criminal standards.
As it stands, there is no unbiased real-time channel for victims to report suspected medical crimes as they are happening. Medical boards are slow. Hospital grievance systems are internal. Civil litigation is expensive.
Law enforcement often does not know how to evaluate medically complex allegations. Agencies disclaim authority. Politicians ask no questions. The result is a justice gap so large that white coats have become shields from accountability and institutional leaders operate above the law.
No profession should place a person above the law.
A medical license should not function as immunity. A hospital system should not be able to investigate itself as the default path. A medical record should not become a weapon that follows a patient from office to office, converting unverified assumptions into barriers to care. And no parent should be told, directly or indirectly, that the only available option is to watch a child decline while every institution points somewhere else.
We need an independent pathway to report suspected medical crimes, preserve evidence, obtain outside review, and trigger referral to the appropriate investigative authority when criminal conduct is occurring.
That pathway must be separate from the medical institutions being accused. It must include patient-submitted evidence. It must protect whistleblowers, patients, parents, and ethical clinicians. And it must operate in real time, because some harms cannot wait for a six-month committee review.
What a Functioning System Would Do
The solution is not complicated.
Create a documented public intake channel for suspected parasitic, fungal, mold-related, and environmental biological health threats.
Require agencies that disclaim authority to identify the agency that does have authority and transfer the report instead of abandoning the citizen.
Expand access to competent diagnostic evaluation, including parasitology expertise, fungal evaluation where medically indicated, and environmental-health review where source exposure is plausible.
Protect essential diagnostic testing and reference-laboratory capacity during public-health emergencies so that one crisis does not erase the country’s ability to detect another.
Require congressional oversight of diagnostic access, public-health surveillance gaps, reimbursement incentives, conflict-of-interest protections, and agency failure to receive citizen-submitted evidence.
Require healthcare reform initiatives, including MAHA-aligned efforts, to include affected patients, parents, independent subject-matter experts, and clinicians who are protected from retaliation for participating honestly.
Create an independent criminal-reporting pathway for suspected medical abuse, evidence suppression, retaliatory charting, record falsification, and other medically complex misconduct that may require law-enforcement review.
These are not radical demands. They are the minimum conditions of a public-health system that claims to protect life.
The Door Must Open
America does not need another slogan about protecting families. It needs a working door.
A mother should not have to become a public-health investigator to get her child evaluated. A family should not have to call every agency in government only to be told that no one has authority. A country that spends more on healthcare than any other nation should not leave families begging for basic diagnostic pathways.
The People’s Dossier, Part I, was only the first layer. More documentation will follow. But the core question is already visible: when a high-resource nation spends more and more while families report less and less
access to meaningful evaluation, who is being protected?
When every agency says “no authority,” the problem is no longer the family.
The problem is the system.
And the system must be forced back into alignment with its most basic purpose: protecting human life.
MAHA has opened an important door. But if that door is guarded by the same institutions patients are reporting, reform will fail before it begins. Healthcare reform cannot be written by industry, filtered by agencies, softened by political offices, and then handed back to suffering families as if they were consulted.
Patients are the missing evidence.
Until the harmed can speak without being filtered by the institutions they are reporting, America will keep mistaking institutional comfort for public health.
Billie Glazier is an American mother, advocate, and former critical-care paramedic. She has decades of higher education and served as a certified firefighter, Haz-Mat instructor, and she taught advanced life-support to healthcare professionals at every level. She now fights to save her family and other Americans abandoned in crisis, in collaboration with affected individuals through R123, an emerging movement built around the three pillars of ethical care. #Stand_and_Roar
Opinions do not reflect the views and opinions of ALPolitics.com. ALPolitics.com makes no claims nor assumes any responsibility for the information and opinions expressed above.